Two years after being diagnosed with T1D at age 15, Kim Beaney was diagnosed with a thyroid condition. That was 50 years ago.
“When I was diagnosed with thyroid disease,” Beaney remembers, her doctor told her to take a pill every day, “so that was a no-brainer.” She’s had many ups and downs over her 52 years with T1D, but keeping her underactive thyroid in check has been relatively simple in comparison. As a result, she said, “Thyroid disease has never bothered me like my diabetes has.”
Beaney, who lives in southern California, is not alone. Thyroid disease and T1D are commonly linked as the two most prevalent autoimmune conditions globally. Just as the immune system can attack the pancreas in T1D, it can also target the thyroid gland. However, not all thyroid issues are autoimmune, meaning some people with T1D may have a thyroid condition that’s not autoimmune-related.
What does the thyroid gland do?
The thyroid is a small gland shaped like a butterfly, located at the base of your neck. It controls hormones that affect how your body uses proteins, fats, and carbohydrates for energy.
The thyroid gland makes and releases two main hormones: T3 (triiodothyronine) and T4 (thyroxine). Together, they’re often called “thyroid hormone.” Your body controls these hormones through a feedback loop that helps to regulate body temperature, heart rate, and blood pressure.
Two other hormones that interact with the thyroid and help it function are:
- thyrotropin-releasing hormone (TRH), which is made by the hypothalamus, and
- thyroid-stimulating hormone (TSH), which is made by the pituitary gland.
What is a thyroid disorder?
There are a variety of conditions that cause overproduction or underproduction of thyroid hormones in the body. The two most common types are:
“When there is an issue with the thyroid, it means it is either producing too much thyroid hormone or too little,” said Dana Roseman, who has lived with T1D for nearly three decades and is director of technology and research at Integrated Diabetes Services. “In either case, the person with thyroid disease will have symptoms associated with too much or too little energy, and more, depending on the condition.”
Leaving thyroid disease untreated can result in serious health risks, especially when combined with T1D.
What are the common symptoms of thyroid conditions?
While hypothyroidism and hyperthyroidism both affect the thyroid, they are different conditions with a variety of causes and symptoms.
With hyperthyroidism (or an overactive thyroid), common signs and symptoms include:
- weight loss (despite increased appetite)
- tachycardia (high heart rate) or palpitations
- heat intolerance
- excessive sweating
- tremors and nervousness
- diarrhea
- muscle weakness
- fatigue
- insomnia
- irritability
- protruding eyes (in the case of Graves’ disease)
- thyroid enlargement or goiter
With hypothyroidism (or an underactive thyroid), common signs and symptoms include:
- fatigue
- weight gain (despite normal or decreased appetite)
- cold intolerance
- constipation
- dry skin/hair
- hair loss
- depression
- cognitive slowing
- bradycardia (low heart rate)
- swelling of skin/tissues (myxedema)
- menstrual irregularities
What tests are used to diagnose thyroid dysfunctions?
Symptoms of thyroid conditions will often lead people to see a healthcare provider. Lab testing and a physical exam of the thyroid will help to rule out any concerns. With T1D, thyroid function testing is suggested on a yearly basis.
Dr. Anira Iqbal, associate staff endocrinologist at the Cleveland Clinic, explained that the most commonly ordered thyroid tests are as follows:
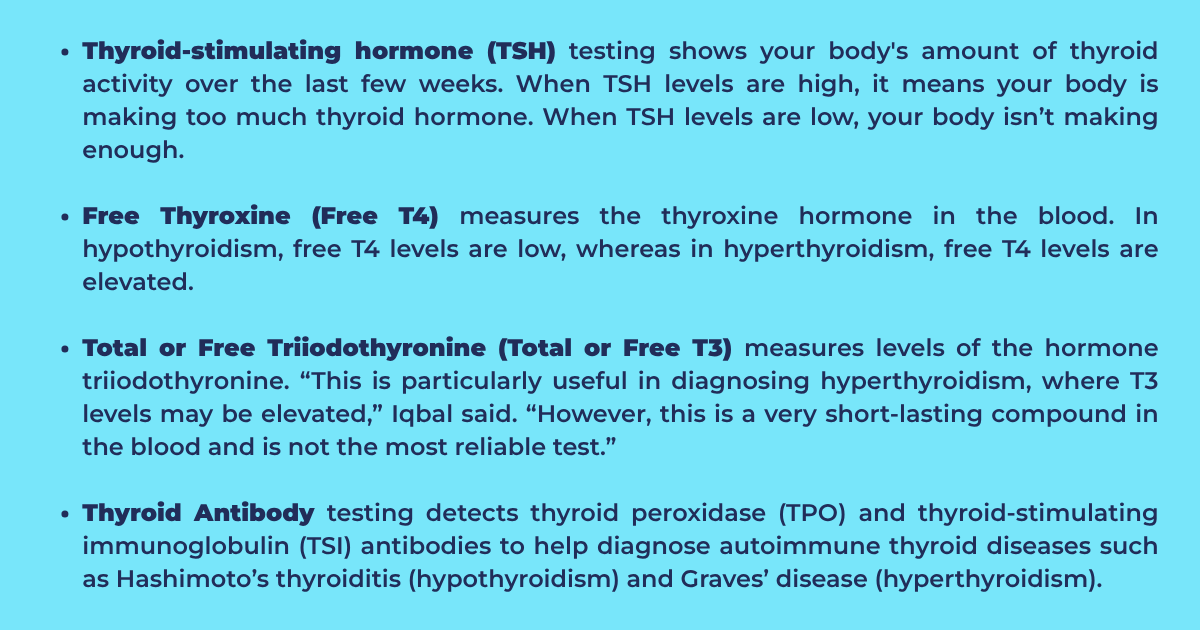
Imaging tests like thyroid ultrasound are sometimes used to assess the thyroid’s size and shape. This can help a provider diagnose various conditions that can affect thyroid health.
What type of thyroid conditions are most common with T1D?
”T1D can be associated with both hypothyroidism and hyperthyroidism,” Iqbal said, with hypothyroidism being more common. Among those living with T1D, Hashimoto’s is the most prevalent cause of hypothyroidism.
According to the American Thyroid Association, women are five to eight times more likely than men to have thyroid issues.
A 2023 study found that 1 in 5 children with T1D have anti-thyroid antibodies at diagnosis, more frequently in girls than boys. Estimates vary, but as many as 1 in 3 people with T1D may have an autoimmune thyroid condition (Hashimoto’s thyroiditis or Graves’ disease), according to another study.
Is there a genetic connection between T1D and thyroid conditions?
Two common conditions, Hashimoto’s thyroiditis (hypo) and Graves’ disease (hyper), are autoimmune thyroid conditions that are more common in people with T1D. “Both of these conditions frequently occur together and are seen in families,” explained Iqbal, “indicating an underlying genetic predisposition.”
“Autoimmune diseases tend to ‘cluster’ together in folks that have a genetic predisposition for developing these conditions,” said Roseman, who lives with Hashimoto’s disease and T1D. Due to the prevalence of thyroid disease in those living with T1D, the American Diabetes Association (ADA) recommends regular thyroid autoantibody screening.
How does having a thyroid condition affect T1D management?
Well-managed thyroid disease can have minimal impact on T1D, such as in Beaney’s and Roseman’s experiences with Hashimoto’s disease. Still, unmanaged thyroid disease can make it more challenging to balance both conditions.
“Thyroid disease can have a lot of negative effects that really impact energy levels, weight management, sleep patterns, heat tolerance, mental health (depression and anxiety levels go up), dry skin, and more,” Roseman said. “Weight gain or loss, lack of energy, and insomnia can all impact insulin needs and requirements. Not to mention just feeling ‘bad’ can decrease motivation for well-managed T1D.”
In some cases, thyroid conditions can be affected by changes in age or medications. Roseman cautioned, “Monitoring is super important, especially during pregnancy, puberty, menopause, and other times of major body changes.”
With T1D, hypothyroidism can lead to more frequent low glucose episodes. According to Iqbal, it may also raise blood lipid (fat) levels, causing dyslipidemia, which can negatively impact heart health. On the other hand, hyperthyroidism can cause high glucose levels due to increased insulin resistance and increased glucose release by the liver. In turn, this can affect cardiovascular health.
What are the treatments?
Hypothyroidism and hyperthyroidism are different conditions, so their treatments are different, too. Symptoms may vary between people, and therapies are tailored to individual needs.
Medications are prescribed to treat severe or significant symptoms of hypothyroidism, Iqbal said, with the gold standard being an oral medication called Synthroid or levothyroxine (a synthetic version of T4).
In cases of hyperthyroidism, Iqbal said, the course of therapy depends on the underlying cause and may include:
Antithyroid drugs to stop the overproduction of thyroid hormone
Radioactive Iodine (RAI) to treat Graves’ disease or toxic nodular goiter, typically followed by lifelong thyroid hormone replacement
Thyroidectomy, or the surgical removal of the thyroid gland, followed by lifelong thyroid hormone replacement
Symptomatic management to treat heart rate, blood pressure, and issues with tremors
The good news is that most thyroid conditions are very treatable. In Beaney’s case, she takes a tablet every day and gets her blood drawn once every three months. Lab results inform necessary changes in medication doses.
If I choose to leave thyroid issues untreated, what happens?
Untreated thyroid issues can have serious health consequences, especially for those living with T1D. “Patients may experience anxiety, insomnia, and tremors,” Iqbal said. Leaving thyroid issues untreated can also impact mental health and lead to a variety of symptoms, including depression, anxiety, and even psychosis in some cases, she said.
Joanne Milo, who writes The Savvy Diabetic blog, was diagnosed with thyroid disease in 1978 and, like Beaney, immediately started on Synthroid (levothyroxine) to treat her hypothyroidism. She was then 28 and had been living with T1D for 13 years.
“I don’t remember much difficulty finding the correct dosing, and it remained very stable for many years,” Milo said. “My symptoms were mostly fatigue and challenges to hold my weight steady.”
Milo, now 70, switched in recent years to the drug Tirosint, a thyroid medication that doesn’t contain sugars or gluten starch. “I’ve never left it untreated,” she said. “But if I did, I’m sure my moods would tank and my energy would go to zero, and I’d guess it would impact my glucose management from the physical stress.”
For Roseman, Hashimoto’s disease has likewise been manageable on top of her T1D. “It goes along with my approach to T1D,” she said. “A well-managed chronic condition does not have to include complications or negative consequences.”